CME information and disclosures
To see contributor disclosures related to this article, hover over this reference: [1]
Physicians may earn CME/MOC credit by searching for an answer to a clinical question on our platform, reading content in this article that addresses that question, and completing an evaluation in which they report the question and the impact of what has been learned on clinical practice.
AMBOSS designates this Internet point-of-care activity for a maximum of 0.5 AMA PRA Category 1 Credit(s)™. Physicians should claim only credit commensurate with the extent of their participation in the activity.
For answers to questions about AMBOSS CME, including how to redeem CME/MOC credit, see "Tips and Links" at the bottom of this article.
Summary
The well-child visits are a vital component of pediatric and public health care, allowing for the prevention of disease through immunizations and anticipatory guidance, and early detection of existing individual health issues that require further follow-up. The schedule starts shortly after birth with the first well-child examination conducted at 3–5 days of age. The first 36 months of life is a time of rapid growth and development and children should be closely monitored with a series of regularly scheduled visits at gradually increasing intervals (from every 2 months to every 6 months). From the age of 3 years, children are assessed annually. Important components of the well-child check-up include age-specific screening recommendations, history taking and physical examination, growth and development assessment (including developmental milestones), administering immunizations, and proactive anticipatory guidance for children.
Overview
Schedule [2][3]
-
Neonatal visits
- 3–5 days after birth
- Another visit by 1 month of age (typically at 2 weeks or 1 month)
- During the first three years: at 2, 4, 6, 9, 12, 15, 18, 24, and 30 months of age
- 3 years and older: annual visits
Approach
Perform the following at every well-child visit.
- Review the child's:
- Past medical history, including any active medical issues
- Results of pediatric screening questionnaires (e.g., developmental surveillance, risk assessments)
- Vital signs and growth charts
- Perform a thorough review of systems and physical examination.
- Recommend and discuss age-appropriate:
- Immunizations according to the ACIP schedule
- Pediatric screening studies
- Pediatric anticipatory guidance
- Arrange the following:
- Further evaluation for abnormal findings, e.g., studies, treatment, follow-up
- The next well-child visit appointment
- For children ≥ 11 years of age, see also “Adolescent health care.”
A sports physical, or preparticipation examination, involves additional history and physical examination components. [4]
Overview of visits by age [3]
The following tables are an outline of the recommended content of well-child checks for healthy children with no additional risk factors identified. If additional risk factors are identified at any point (e.g., risk factors for pediatric hypertension, risk factors for lead toxicity), more frequent screenings (e.g., at every visit) may be required.
Screen children once between birth and 21 years of age for risk factors for hepatitis B and if risk factors are present, send HBV serology, even if the child has been vaccinated. [3]
Infancy
| Overview of recommendations for infants by age [3] | |
|---|---|
| Recommended screening/assessments at visit | |
| All ages |
|
| 3–5 days |
|
| By 1 month |
|
| 2 months |
|
| 4 months |
|
| 6 months |
|
| 9 months |
|
| 12 months |
|
Screen children for risk factors for dental caries once at 6 months and at 9 months. If the child does not have an established dentist by the recommended age of 12 months, continue to assess for risk factors and the need for fluoride varnish through 6 years of age.[3]
Toddlers and preschool children
| Overview of recommendations for toddlers and preschool children by age [3] | |
|---|---|
| Recommended screening/assessments at visit | |
| All ages |
|
| 15 months |
|
| 18 months |
|
| 24 months |
|
| 30 months |
|
| 3 years |
|
| 4 years |
|
School-aged children and adolescents
| Overview of recommendations for school-aged children by age [3] | |
|---|---|
| Recommended screening/assessments at visit | |
| All ages |
|
| 5 years |
|
| 6 years |
|
| 7 years |
|
| 8 years |
|
| 9 years |
|
| 10 years |
|
| ≥ 11 years |
|
Growth
Approach [7][8]
- Obtain all indicated growth parameters at each visit.
-
Plot measurements on a gender-specific growth chart.
- < 2 years: WHO growth charts [7]
- ≥ 2 years: CDC growth charts [9]
- Special patient populations: Use a condition-specific growth curve, if available. [10]
- Calculate the mid-parental height in order to [10]
- Determine the expected adult height based on genetic potential [11]
- Compare current growth percentiles to the expected growth percentiles
- Track growth over time to identify pediatric growth patterns.
")
")
")
")
")
")
")
")
")
")
Pediatric growth patterns [8]
-
Normal pediatric growth
- Proportionate growth parameters
- Growth parameters that follow closely to a percentile curve [8][10]
- Expected height within 2 standard deviations (i.e., 10 cm or 4 inches) of the mid-parental height [10]
-
Abnormal pediatric growth
- Values that deviate ≥ 2 standard deviations from the mean, i.e. < 3% or > 97% percentiles
- Crossing ≥ 2 major percentile lines on the growth curve [8]
- Deviating > 10 cm (4 inches) from the mid-parental height [10]
- Disproportionate parameters
To help identify abnormal growth patterns, compare the child's growth parameter percentiles to their expected adult height (i.e., mid-parental height). [10][11]
Children < 2–3 years may cross major percentiles, but after this time should track consistently. [8]
Growth parameters [8]
| Pediatric growth parameters [8][10] | |||
|---|---|---|---|
| Indications and method | Expected trends | Abnormal growth | |
| Head circumference-for-age |
|
|
|
| |||
| Linear growth [8] |
|
|
|
| Weight-for-age measurement |
|
|
|
| Weight-for-length OR BMI |
|
|
|
In children with normal development, examination, and no evidence of rapidly increasing FOC, macrocephaly is most likely benign (e.g., due to familial macrocephaly). If parental FOC suggests a genetic contribution to a child's macrocephaly, management involves reassurance and observation. [23]


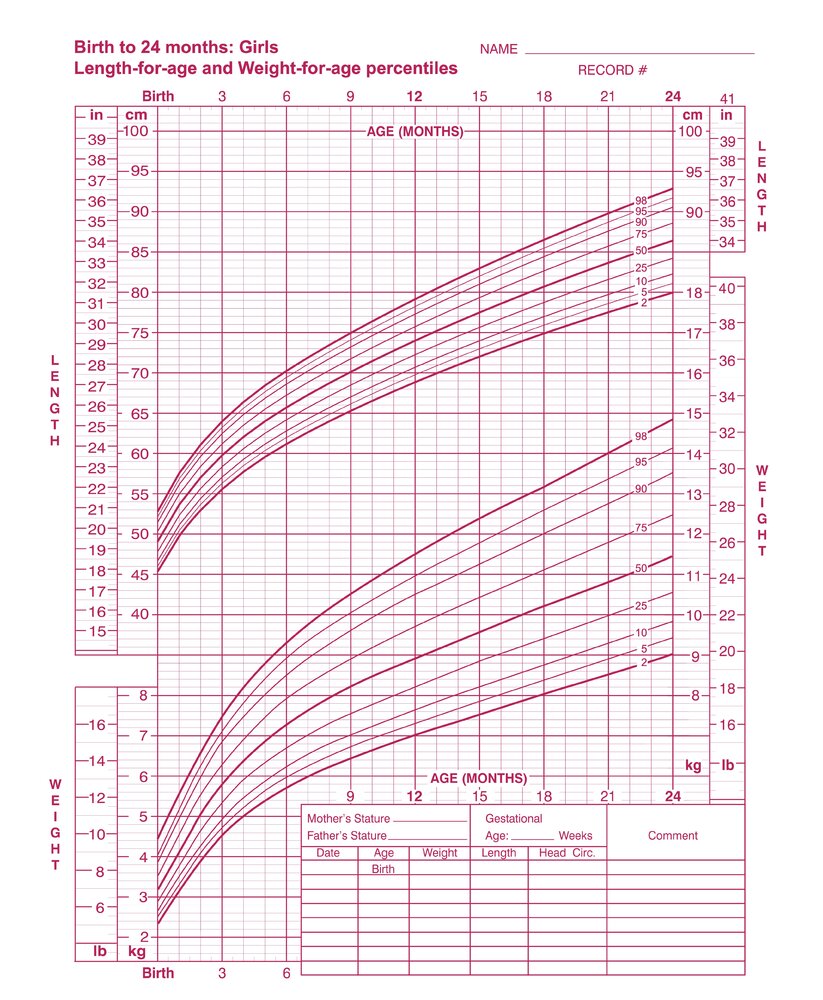
This image is an adaptation. Source of original image: Centers for Disease Control and Prevention. Original title: “Birth to 24 months: Girls Length-for-age and Weight-for-age percentiles”. Created by: Centers for Disease Control and Prevention. Licensed under Public Domain. Modifications to original image: CDC logo removed by request.
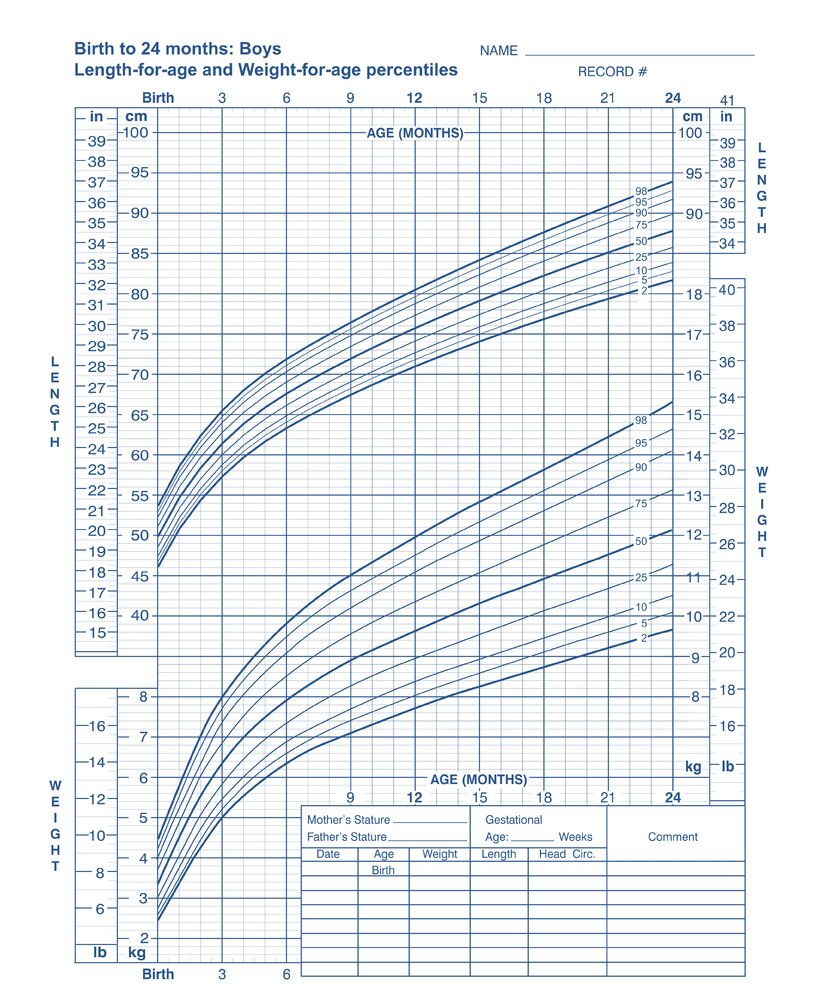
This image is an adaptation. Source of original image: Centers for Disease Control and Prevention. Original title: “Birth to 24 months: Boys Length-for-age and Weight-for-age percentiles”. Created by: Centers for Disease Control and Prevention. Licensed under Public Domain. Modifications to original image: CDC logo removed by request.
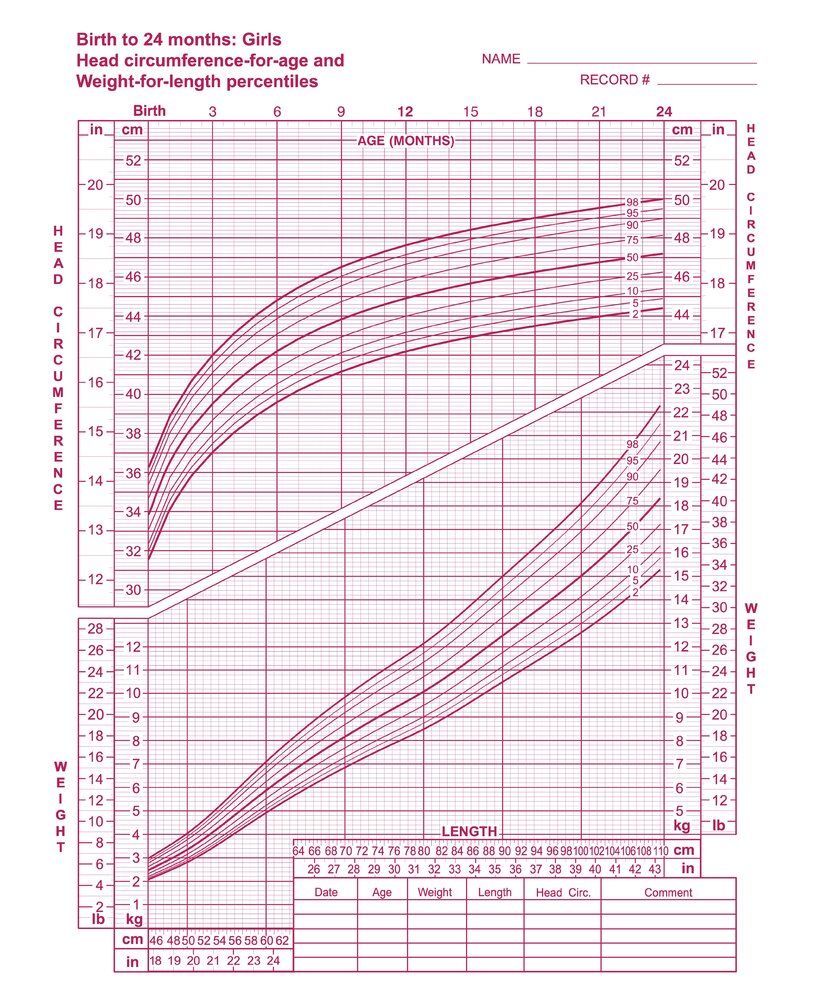
This image is an adaptation. Source of original image: Centers for Disease Control and Prevention. Original title: “Birth to 24 months: Girls Head circumference-for-age and Weight-for-length percentiles”. Created by: Centers for Disease Control and Prevention. Licensed under Public Domain. Modifications to original image: CDC logo removed by request.
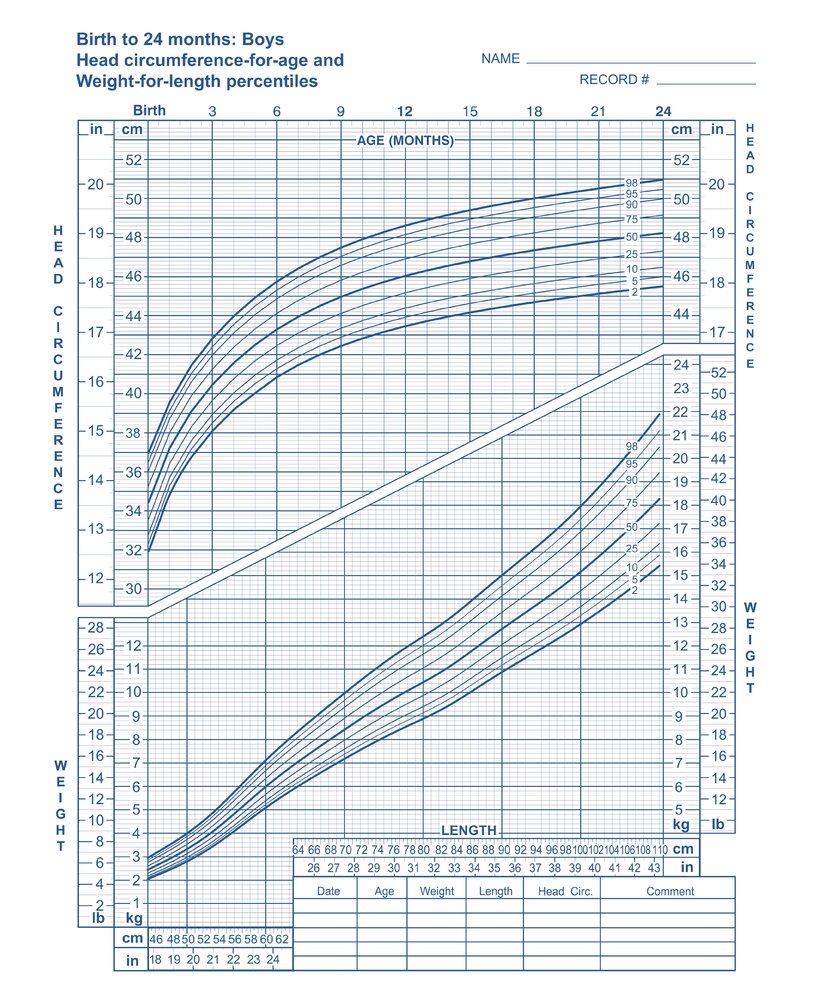
This image is an adaptation. Source of original image: Centers for Disease Control and Prevention. Original title: “Birth to 24 months: Boys Head circumference-for-age and Weight-for-length percentiles”. Created by: Centers for Disease Control and Prevention. Licensed under Public Domain. Modifications to original image: CDC logo removed by request.
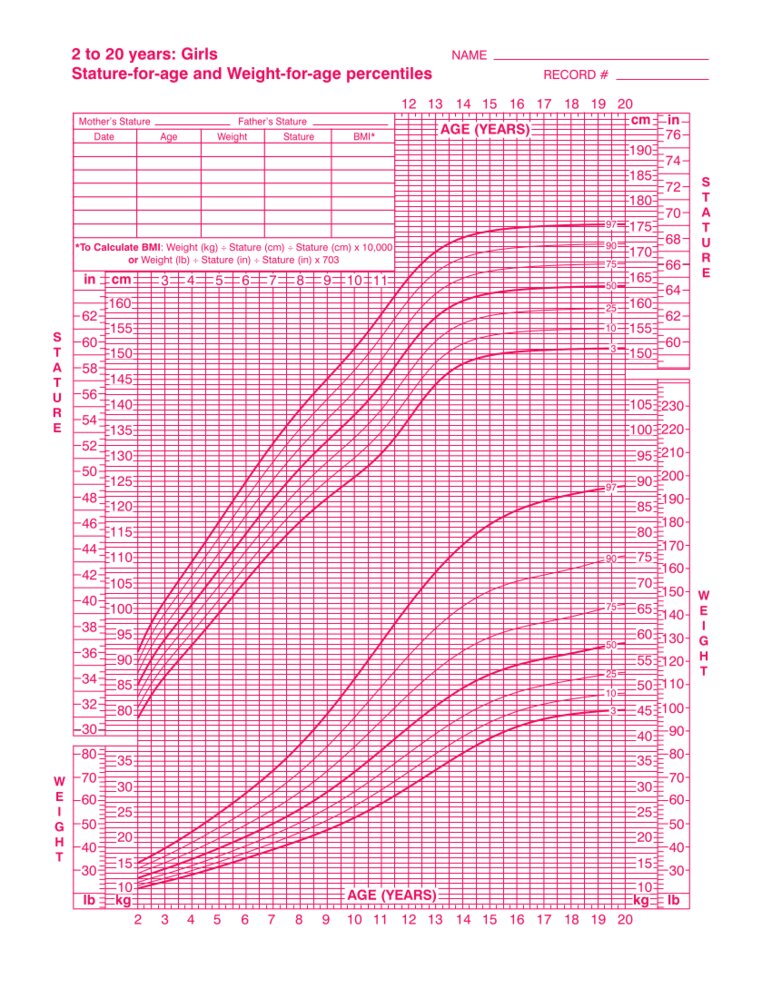
This image is an adaptation. Source of original image: CDC. Original title: “2 to 20 years: Girls, Stature-for-age and Weight-for-age percentiles”. Created by: Centers for Disease Control and Prevention, National Center for Health Statistics. Licensed under Public Domain. Modifications to original image: CDC logo removed by request.
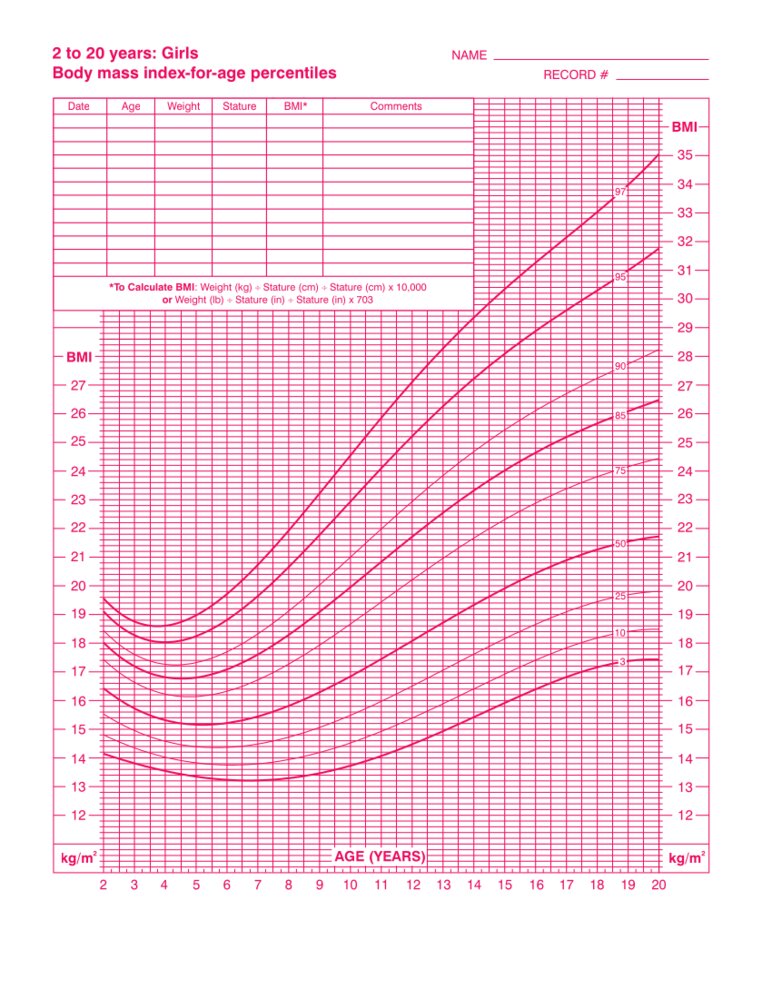
This image is an adaptation. Source of original image: CDC. Original title: “2 to 20 years: Girls, Body mass index-for-age percentiles”. Created by: Centers for Disease Control and Prevention, National Center for Health Statistics. Licensed under Public Domain. Modifications to original image: CDC logo removed by request.
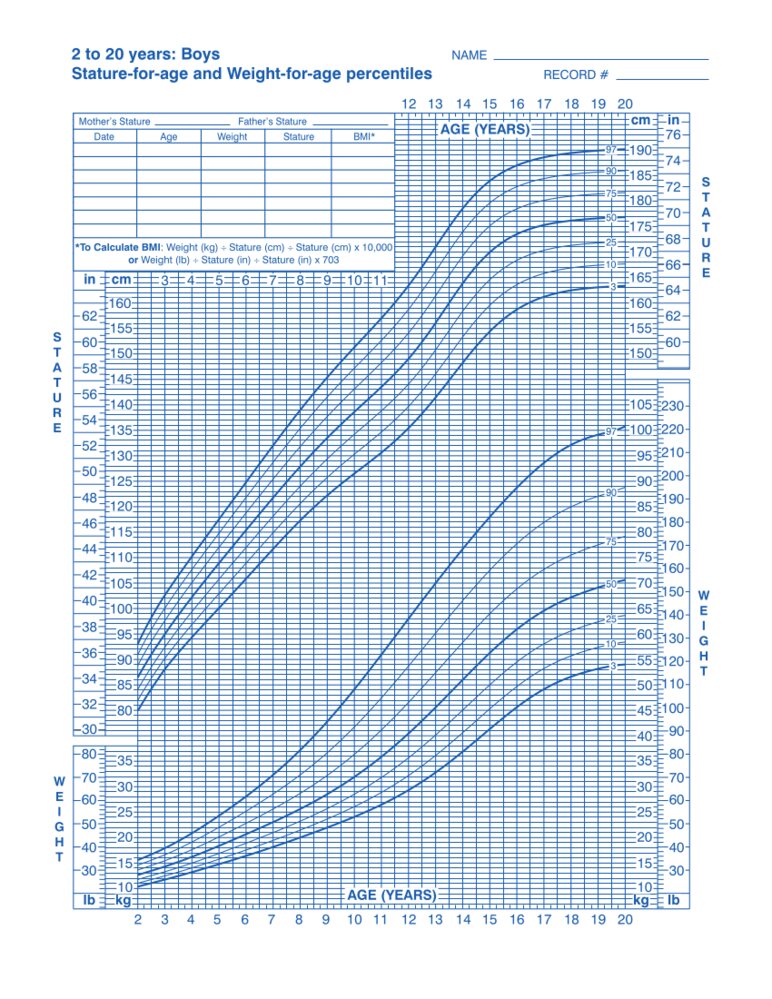
This image is an adaptation. Source of original image: CDC. Original title: “2 to 20 years: Boys, Stature-for-age and Weight-for-age percentiles”. Created by: Centers for Disease Control and Prevention, National Center for Health Statistics. Licensed under Public Domain. Modifications to original image: CDC logo removed by request.
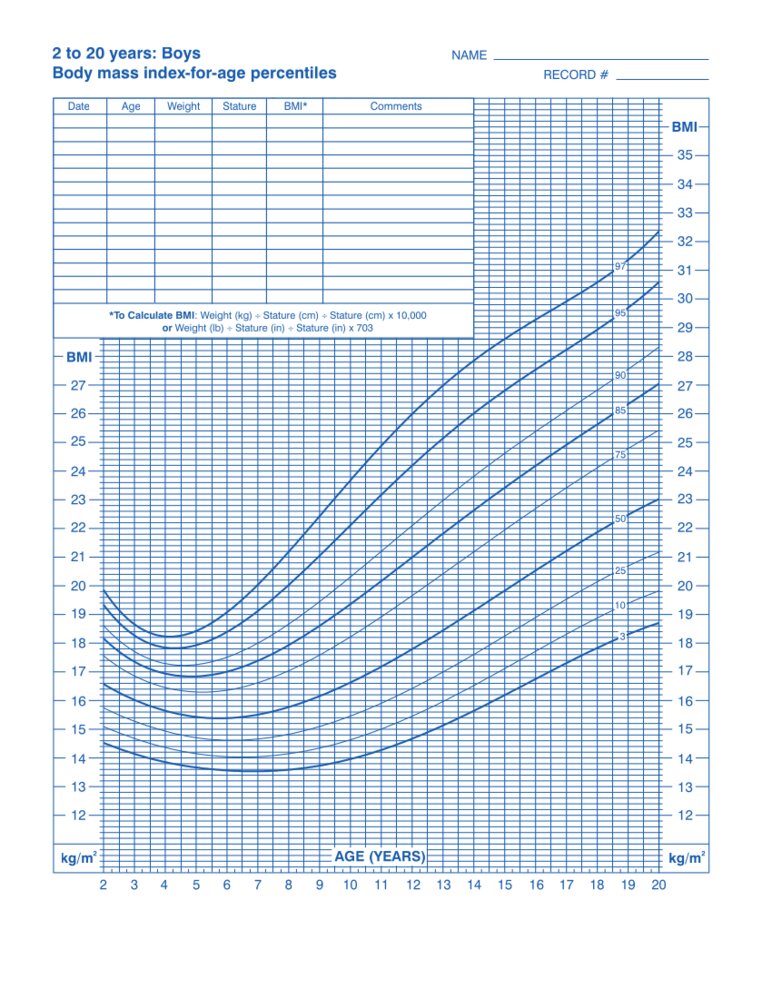
This image is an adaptation. Source of original image: CDC. Original title: “2 to 20 years: Boys, Body mass index-for-age percentiles”. Created by: Centers for Disease Control and Prevention, National Center for Health Statistics. Licensed under Public Domain. Modifications to original image: CDC logo removed by request.
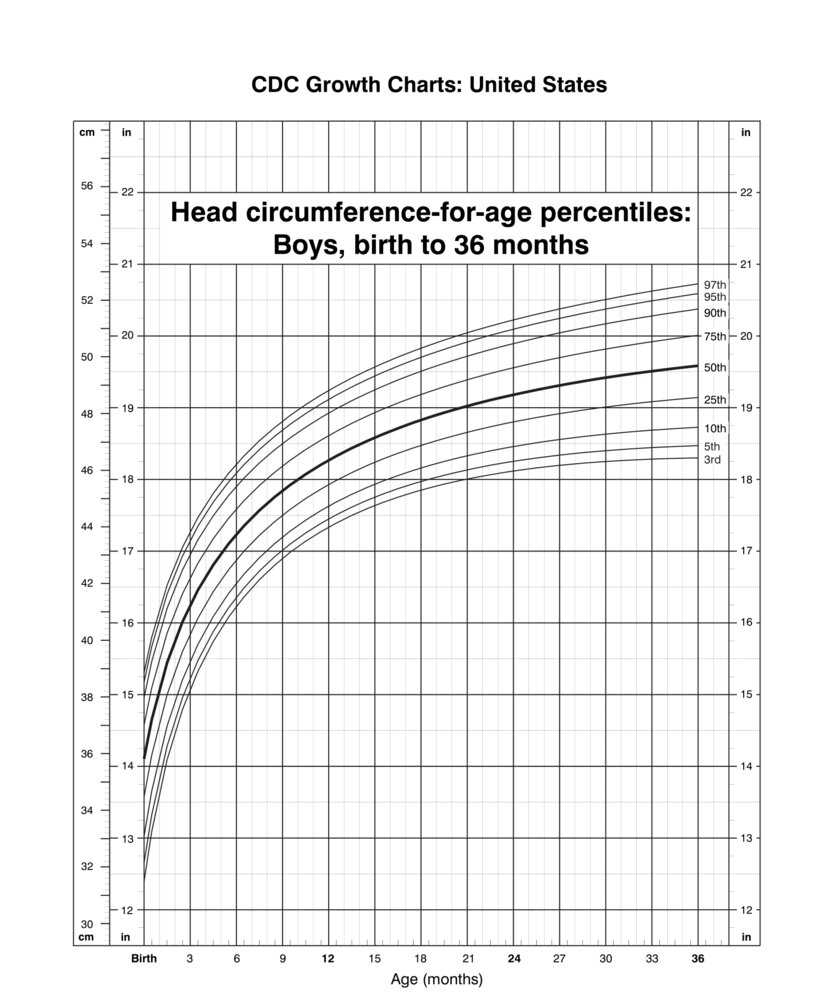
This image is an adaptation. Source of original image: CDC. Original title: “Head circumference-for-age percentiles: Boys, birth to 36 months”. Created by: National Center for Health Statistics; National Center for Chronic Disease Prevention and Health Promotion. Licensed under Public Domain. Modifications to original image: CDC logo removed by request.
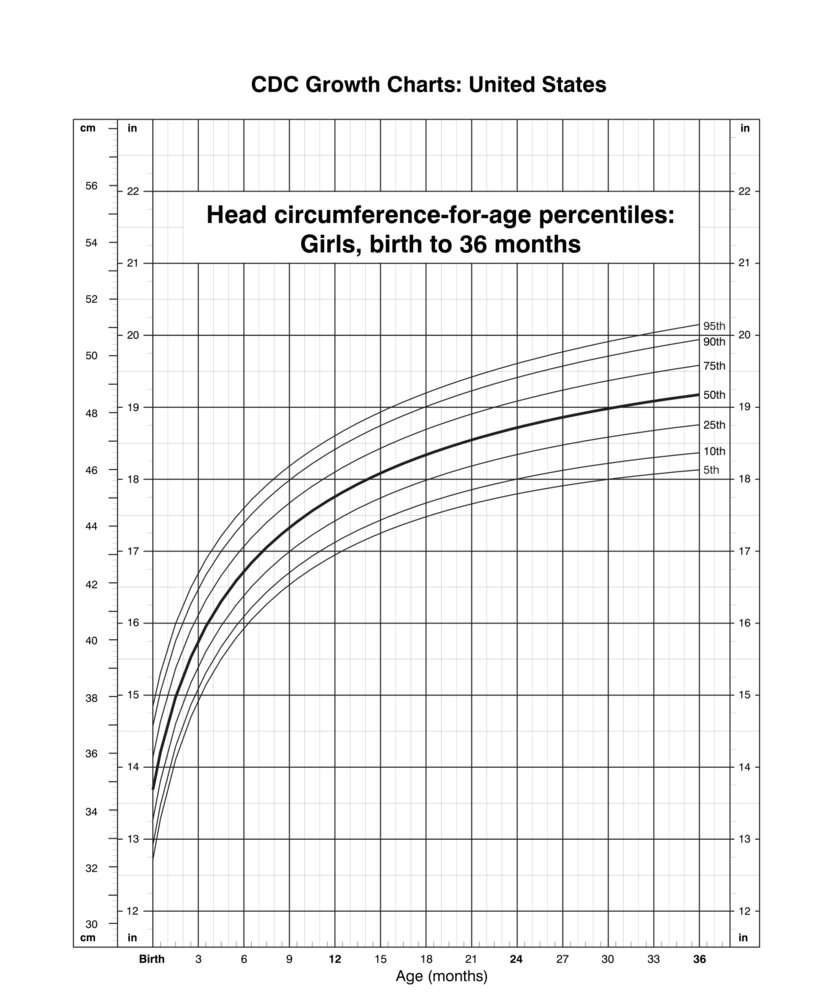
This image is an adaptation. Source of original image: CDC. Original title: “Head circumference-for-age percentiles: Girls, birth to 36 months”. Created by: National Center for Health Statistics; National Center for Chronic Disease Prevention and Health Promotion. Licensed under Public Domain. Modifications to original image: CDC logo removed by request.
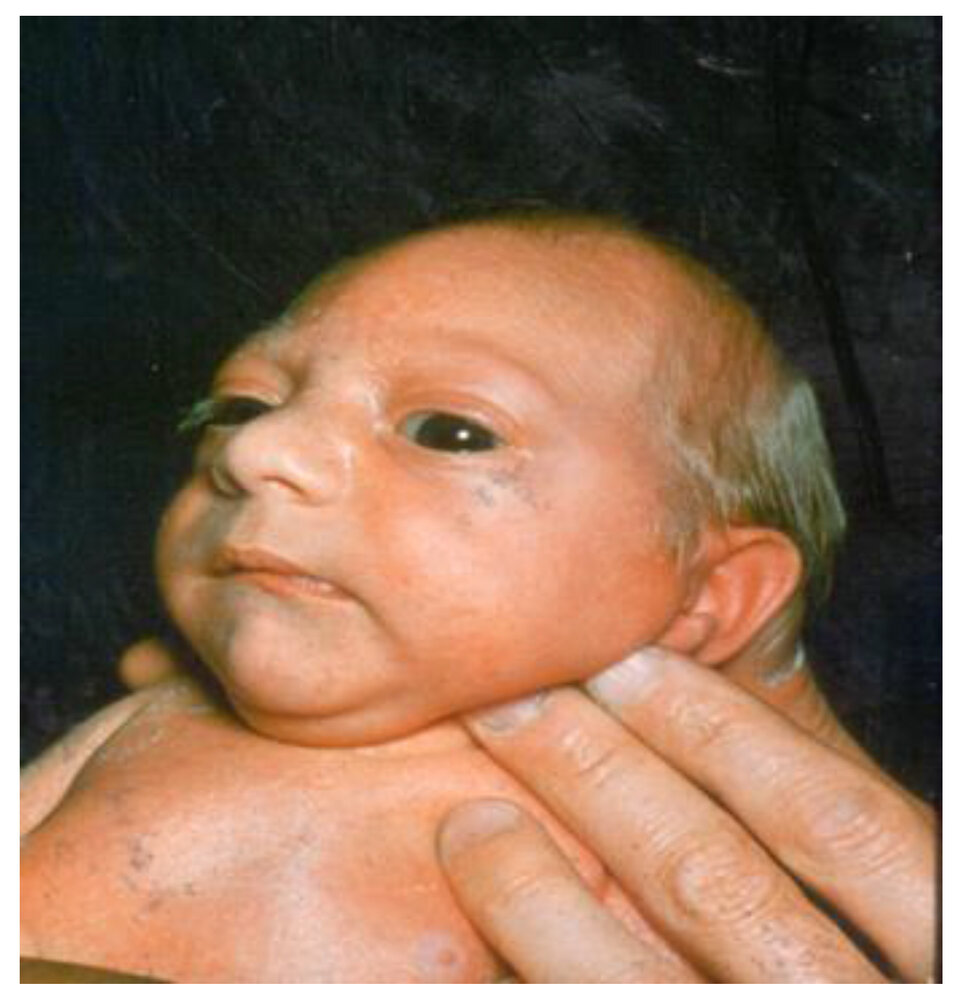
The head circumference of this newborn infant is more than two standard deviations below the mean size for age and sex, consistent with congenital microcephaly.
Source: “Fig 1, in: Microcephaly” by Hanzlik E, Gigante J, Children, licensed under CC BY 4.0.

Macrocephaly and large earlobes.
Source: “File:Fragx-2.jpg” by Peter Saxon, Wikimedia Commons, licensed under CC BY-SA 4.0. Modifications: Eyes pixelated.
{kind=link}
Screening
- Routine screening allows early detection and early treatment of common healthcare problems.
- This section includes recommendations from the American Academy of Pediatrics (AAP) and the US Preventative Services Task Force (USPSTF).
- For additional recommendations (e.g., sexual health screening, substance use) in older children, see “Adolescent health care.”
Physical exam screening
- See also “Pediatric growth” for recommendations on monitoring height and weight.
| Pediatric physical exam screening recommendations [2][3][24] | ||||
|---|---|---|---|---|
| Conditions to screen | Recommended ages | Method of screening | Actions for abnormal findings | |
| Pediatric hearing screening [25][26][27] |
|
|
|
|
| Pediatric vision screening [24][29][30][31] |
|
|
|
|
|
|
|||
|
|
|||
| Scoliosis screening [6][37][38][39] |
|
|
|
|
| Pediatric hypertension screening [6][40] |
|
|
|
|
Vision screening identifies conditions, e.g., cataracts, strabismus (in infants ≥ 4 months of age), amblyopia, that require interventions to prevent permanent vision loss. During a fundoscopic evaluation, the absence of a red reflex and/or the presence of leukocoria requires urgent ophthalmology referral and further evaluation. [41]
Hearing loss can be mistaken for other conditions. Always perform a pediatric hearing screening in children with communication disorders, neurodevelopmental disorders, and behavioral problems. [42][43]
Screening studies
Screening studies for anemia and dyslipidemia are required at set ages, regardless of risk factors. Screening studies for hepatitis B, lead toxicity, tuberculosis, and sudden cardiac death are only performed in patients with confirmed risk factors.
| Recommended pediatric screening studies [2][3][24] | ||||
|---|---|---|---|---|
| Conditions to screen | Indications for screening | Method of screening | Actions for abnormal findings | |
| Anemia screening |
|
|
|
|
| Hepatitis B screening |
|
|
|
|
| Blood lead screening [44][45] |
|
|
|
|
| Pediatric dyslipidemia screening [48] |
|
|
|
|
| Tuberculosis (TB) risk assessment [49] |
|
|
|
|
| Sudden cardiac death [50] |
|
|
|
|
Developmental screening
See also “Child development and milestones.”
| Pediatric developmental screening recommendations [2][3] | ||||
|---|---|---|---|---|
| Conditions to screen | Recommended ages | Method of screening | Actions for abnormal findings | |
| Child developmental milestone screening [51] |
|
|
|
|
|
|
|
||
| Autism screening [43] |
|
|
|
|
Mental and social health screening
| Pediatric mental and social health screening recommendations [2][3] | ||||
|---|---|---|---|---|
| Conditions to screen | Recommended ages | Method of screening | Actions for abnormal findings | |
| Parental postpartum depression screening |
|
|
|
|
| Social determinants of health [53][54] |
|
|
|
|
| Behavioral, social, and emotional disorders screening |
|
|
|
|
| Anxiety [55] |
|
|
||
| Depression and suicide screening [56] |
|
|
||
This calculator is provided by the third-party QXMD, who is solely responsible for its content and functionality.
Created by: QxMD.
History and examination
History [24]
- Review the patient's medical and family history.
- Perform a pediatric review of systems, including
- Constitutional symptoms (e.g., changes in weight, fevers)
- Sleep-related concerns (e.g., deficient sleep, night terrors, napping, snoring)
- Dietary concerns (e.g., picky eating, unhealthy eating habits, eating disorders)
- Elimination disorders (e.g., daytime continence, encopresis, nocturnal enuresis, constipation in children)
- Menstrual cycles (e.g., menarche, menstrual cycle abnormalities)
- School-related concerns (e.g., ADHD symptoms, learning disorders, academic problems)
- Behavioral concerns (e.g., temper tantrums, anxiety, depression)
- See “Pediatrics: history and physical examination” for more information.
Physical examination [24]
- Perform a thorough physical examination, including age-specific examinations.
- See “Pediatrics: history and physical examination” for further information.
| Age-specific physical examination in children | ||
|---|---|---|
| Age | Recommended evaluation | Possible findings |
| Neonatal |
|
|
| Infants |
|
|
| Toddlers and preschool-aged children |
|
|
| School-aged children and adolescents |
|
|
Normal pediatric vital signs vary greatly by age.
Anticipatory guidance
Anticipatory guidance involves proactive counseling for expected age-appropriate topics (e.g., safety, healthy lifestyles, nutrition, and dental care). See also “Anticipatory guidance for pediatric development.”
Pediatric illness anticipatory guidance
-
Illness prevention
- Advise adherence to recommended immunizations in children.
- Discuss strategies to prevent disease transmission (e.g., hand hygiene, respiratory hygiene), especially around at-risk populations.
- Educate parents of newborns on neonatal umbilical hygiene.
-
Illness management
- Educate parents on signs of illness (e.g., clinical features of neonatal bacterial infection, clinical features of pediatric fever)
- Discuss anticipatory guidance for pediatric fever.
- Give examples of when to:
- Seek emergency care (e.g., signs of respiratory distress, clinical features of dehydration, red flags for pediatric fever)
- Contact the pediatrician's office
- Follow school or childcare guidance on when to return to childcare or school.
Child safety [24][61][62]
-
Sleeping [63]
- Provide counseling on sudden infant death syndrome and prevention of SIDS.
- Educate on proper swaddling: safe sleep swaddling, healthy hip swaddling.
- Secondhand smoke: Advise caregivers on the risks of secondhand smoke and offer assistance with smoking cessation.
-
Child passenger safety: Children ≤ 13 years of age should ride in the back seat in a car safety seat that is approved for their age, weight, and height. ; [2][64][65][66]
- Laws regarding minimum safety requirements for car safety seats vary between states.
- The AAP recommends using car safety seats in the following order; advance to the next seat once the child reaches seat limits:
- Rear-facing with harness: starting at birth until at least 2 years of age
- Forward-facing with harness (convertible or dedicated forward seat)
- Booster seat
- Lap and shoulder seat belts can be used once they fit correctly.
-
Supervision
- Supervision must be provided by a responsible adult who is awake and not under the influence of alcohol or other substances. [67]
- 3–5 years: Continuous supervision is necessary. [68]
- 6–8 years: Supervision is necessary near bodies of water or during risky activities (e.g., climbing). [69]
- Bullying and abuse prevention: Teach verbal children (e.g., ≥ 3 years of age) how to recognize, respond to, and report inappropriate interactions.
-
Street and recreational safety
- Instruct children to wear protective gear when engaging in activities with an increased risk of injury (e.g., cycling, skateboarding).
- Teach children road safety.
-
Water safety: Encourage multiple preventive strategies.
- Do not leave children unattended near bodies of water.
- Consider survival swim lessons at an early age.
- A self-locking fence should be installed around pools.
-
Sun safety
- Advise sun avoidance and protective clothing.
- Use sunscreen in children ≥ 6 months of age.
-
Childproofing the house
-
Pediatric poisoning prevention: Keep the following out of reach of children. [70]
- Potentially harmful household products (e.g., laundry detergent pods, cleaning products)
- Medications (prescription and nonprescription, including vitamins)
- Alcohol containers and nicotine products
- Set water heaters to 120°F (49°C) maximum temperature.
- Firearms should be locked out of reach of children (unloaded with ammunition stored separately).
- Anchoring furniture to walls can prevent accidental crush injuries.
- Keep areas accessible to children (e.g., floors, tables) clear of small objects.
-
Pediatric poisoning prevention: Keep the following out of reach of children. [70]
- Fire safety: Install smoke alarms and formulate a family escape plan.
-
Medication safety for children
- All medications should be stored in a secure location that is out of reach of children.
- Educate caregivers on over-the-counter medications to avoid dosing errors. [71]
- Ensure the medication is approved for the child's age.
- Use single-ingredient medications whenever possible.
- Follow dosing labels; weight-based dosing is preferred over age-based dosing.
- See also “Home management of pediatric fever.”
- Ask about use of complementary and alternative medicine. [72]

Pediatric lifestyle recommendations [24][73]
-
Pacifier use [63][74]
- Consider delaying pacifier use until breastfeeding has been well-established.
- To assist in prevention of SIDS, encourage pacifier use during sleep in infants 1–6 months of age.
- Limit pacifiers after 6 months of age to reduce the risk of otitis media.
- Discontinue pacifiers at 2 to 4 years of age to prevent adverse dental effects (e.g., dental malocclusion).
-
Behavior and discipline
- Discuss age-appropriate behaviors to manage parent expectations.
- Encourage consistency, positive reinforcement, and age-appropriate discipline.
- For persistent behavioral problems (e.g., temper tantrums, aggression), recommend evidence-based parenting programs.
-
Toilet training [75]
- Initiation: At 2.5–3 years of age, when children are developmentally mature enough to begin toilet training. [76]
- Use positive reinforcement.
- Completion: typically by 4 years of age
-
Screen time [24][68][73]
- Children aged < 18 months: Avoid screen time, with the exception of video calls.
- Children aged 18–24 months: Limit screen time solely to educational content.
- Children aged 2–5 years: Restrict sedentary screen time to ≤ 1 hour/day.
- For older children:
- Encourage use of an agreed plan for caregiver supervision, limits on screen time, and scheduled screen-free time.
- Avoid screen time within 1 hour of bedtime and keep devices out of children's bedrooms.
-
Sleep: See also “Counseling on sleep hygiene.” [77]
- 3–5 years: A total of 10–13 hours of sleep is recommended (including naps).
- 6–12 years: Children should get 9–12 hours of sleep; daytime naps should not be forced.
- Physical exercise: Ensure at least 60 minutes of daily physical activity.
- Personal hygiene: Establish good hygiene habits, including hand hygiene, respiratory hygiene, regular bathing; in adolescents, this should also include the use of deodorant.
- Counseling on sexual activity, smoking, alcohol, and drug use: See “Adolescent health care.”
Do not attach pacifiers to sleeping infants or to items that present a suffocation risk (e.g., stuffed animals). [63]
Pediatric nutrition [24][78][79]
A healthy diet is essential for normal growth and development and helps prevent a variety of metabolic and other conditions, such as obesity and type 2 diabetes mellitus.
-
Infant feeding: See also “Infant nutrition.”
- Encourage exclusive breastfeeding for the first 6 months. [24]
- Exclusively breastfed or partially breastfed infants require supplementation.
- Vitamin D from birth until infants meet the recommended daily intake of vitamin D from other food sources
- Iron from 4 months until they meet the recommended daily intake of iron from iron-containing foods [80]
- Introduce complementary foods at 6 months of age if showing signs of complementary feeding readiness.
- In addition to complementary foods, breastmilk and/or formula should be given until 12 months of age.
-
Older children
- Once eating solid foods, a healthy diet consists of [14]
- Three meals and two snacks per day
- Caloric intake appropriate for the child's age and level of activity
- Fruits, vegetables, legumes, beans, grains (preferably whole grain), protein foods, and dairy
- Limited saturated fats, salt, and sugar
- Introduce whole milk (16–24 oz/day) at 12 months of age. [78][81]
- At 24 months of age, switch from whole milk to 1% or skim milk. [82]
- Once eating solid foods, a healthy diet consists of [14]
For children on specialized diets (e.g., for medical indications, vegetarians, vegans), consider referral to a dietitian to ensure proper dietary intake of macronutrients and micronutrients. [83]
Picky eating [84]
-
Definition
- The refusal to eat certain foods, try new foods, or eat sufficient amounts of food
- Often associated with an excessive preference for certain foods
-
Red flags in picky eating that merit further evaluation include:
- Vomiting, diarrhea, or atopy (e.g., eczema)
- Dysphagia (may manifest with coughing, choking, or recurrent lower respiratory tract infections)
- Odynophagia (may manifest with crying while eating)
- Failure to thrive, developmental delay
-
Management: depends on the severity of the condition
-
Normal growth with no red flags
- Diagnostic studies are not indicated.
- Reassure parents and encourage them to continue offering a wide variety of foods.
- Poor growth and/or red flags in picky eating
- Perform a detailed history, including screening for eating disorders.
- Obtain diagnostics studies as indicated.
- Consider caloric supplementation.
- If indicated, make appropriate referral(s).
-
Normal growth with no red flags
Encourage caregivers to offer a variety of foods without pressuring children to eat.
Dental care and caries prevention in children [85][86]
-
General care
- Avoid juices in infants and limit to 4–6 oz (120–180 mL) per day for children ≥ 1 year of age [86][87]
- Introduce a cup at 6 months of age; discourage bottles past 1 year old.
- Before tooth eruption, wipe gums with a clean cloth after meals.
- After tooth eruption
- Brush teeth twice a day with fluoridated toothpaste.
- Floss daily between teeth that touch.
- Encourage dental visits every 6 months beginning with tooth eruption or at 12 months, whichever is first.
-
Additional fluoride [85]
- After tooth eruption: Consider applying fluoride varnish every 3–6 months. [85]
- Consider fluoride supplementation in those who drink fluoride-deficient water. [85][88][89]
Oral health concerns
-
Teething: the physiological process by which an infant's deciduous teeth emerge through the gums
- Usually begins with the lower central incisors between 6 and 10 months of age and ends with the molars at 2–3 years of age [90]
-
Teething syndrome: Manifestations fluctuate with the eruption of teeth and include drooling, irritability, disrupted sleep, and/or swelling/inflammation of the gums.
- Providing infants with a chilled teething ring to chew on safely or applying pressure to the baby's gum using clean fingers or wet gauze can reduce discomfort.
- Systemic analgesics (e.g., acetaminophen, ibuprofen) are reserved for teething pain not effectively managed with conservative interventions.
- Advise parents against using topical numbing treatments due to the risk of adverse effects (e.g., methemoglobinemia). [91]
- Dental malocclusion: Discourage nonnutritive sucking habits, including thumb sucking and pacifier use, beyond 3 years of age. [92]
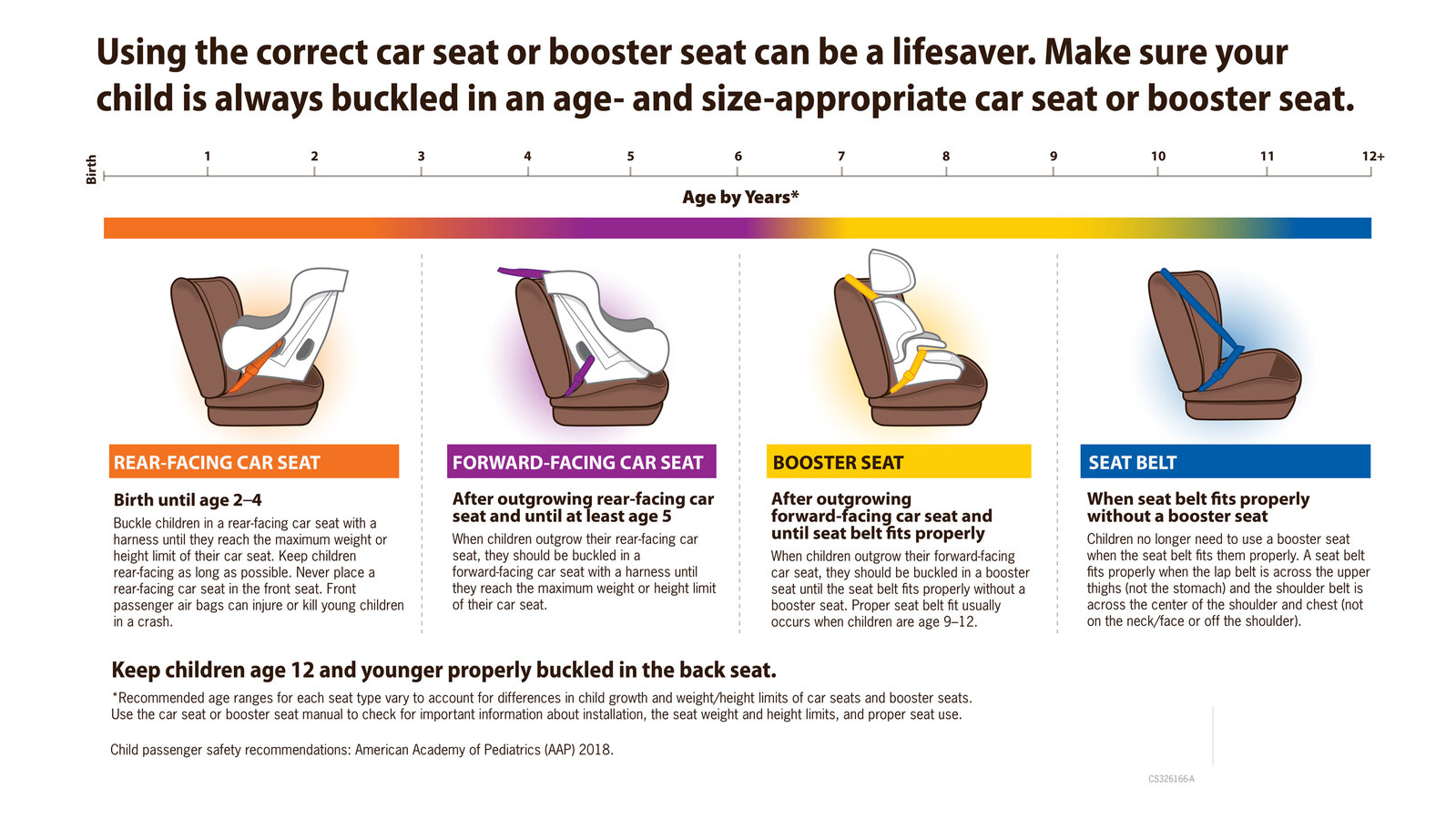
This image is an adaptation. Source of original image: CDC. Original title: “Child car seat booster”. Created by: American Academy of Pediatrics, CDC. Licensed under Public Domain. Modifications to original image: cropped away CDC link + label.
Related One-Minute Telegram
- One-Minute Telegram 111-2024-3/3: Digital interventions help prevent childhood obesity
Interested in the newest medical research, distilled down to just one minute? Sign up for the One-Minute Telegram in “Tips and links” below.
External Resources
References
- Hagan JF, Shaw JS, Duncan PM. "Bright Futures: Guidelines for Health Supervision of Infants, Children and Adolescents, 4th Edition". American Association of Pediatrics. (2017). ISBN: 9781610020220
- "Recommendations for Preventive Pediatric Health Care". https://web.archive.org/web/20230126132131/https://downloads.aap.org/AAP/PDF/periodicity_schedule.pdf. [2022-07-01]
- MacDonald J, Schaefer M, Stumph J. "The Preparticipation Physical Evaluation". Am Fam Physician. 103(9). :539-546. (2021)
- Warner RM, Cleary C, et al. "2025 Recommendations for Preventive Pediatric Health Care: Policy Statement". Pediatrics. (2025)
- Riley M, Morrison L, McEvoy A. "Health Maintenance in School-Aged Children: Part I. History, Physical Examination, Screening, and Immunizations". Am Fam Physician. 100(4). :213-218. (2019)
- "Safety & Prevention". https://web.archive.org/web/20221129190451/https://www.healthychildren.org/english/safety-prevention/Pages/default.aspx. [2022-01-01]
- "Childproofing Your Home- 12 Safety Devices To Protect Your Children". https://web.archive.org/web/20221129185250/https://www.cpsc.gov/safety-education/safety-guides/kids-and-babies/childproofing-your-home-12-safety-devices-protect
- Turner K. "Well-Child Visits for Infants and Young Children". Am Fam Physician. 98(6). :347-353. (2018)
- Moon RY, Carlin RF, Hand I, Task Force on Sudden Infant Death Syndrome and the Committee on Fetus and Newborn. "Evidence Base for 2022 Updated Recommendations for a Safe Infant Sleeping Environment to Reduce the Risk of Sleep-Related Infant Deaths". Pediatrics. 150(1). (2022)
- "Child Passenger Safety: Get the Facts". https://web.archive.org/web/20220919154114/https://www.cdc.gov/transportationsafety/child_passenger_safety/cps-factsheet.html. [2020-10-30]
- Durbin DR, Hoffman BD, Agran PF, et al. "Child Passenger Safety". Pediatrics. 142(5). (2018)
- "Car Seats: Information for Families". https://web.archive.org/web/20221129183812/https://www.healthychildren.org/English/safety-prevention/on-the-go/Pages/Car-Safety-Seats-Information-for-Families.aspx. [2021-12-22]
- Freisthler B, Johnson-Motoyama M, Kepple NJ. "Inadequate child supervision: The role of alcohol outlet density, parent drinking behaviors, and social support". Child Youth Serv Rev. 43. :75-84. (2014)
- "Preschoolers (3-5 years of age)". https://web.archive.org/web/20210319083520/https://www.cdc.gov/ncbddd/childdevelopment/positiveparenting/preschoolers.html
- "Middle Childhood (6-8 years of age)". https://web.archive.org/web/20211003062247/https://www.cdc.gov/ncbddd/childdevelopment/positiveparenting/middle.html. [2021-02-22]
- AAP. "Childproofing Your Home". Pediatric Patient Education. (2021)
- Yin HS, Neuspiel DR, Paul IM, et al. "Preventing Home Medication Administration Errors". Pediatrics. 148(6). (2021)
- McClafferty H, Vohra S, Bailey M, et al. "Pediatric Integrative Medicine". Pediatrics. 140(3). :e20171961. (2017)
- Locke A, Stoesser K, Pippitt K. "Health Maintenance in School-Aged Children: Part II. Counseling Recommendations". Am Fam Physician. 100(4). :219-226. (2019)
- Sexton S, Natale R. "Risks and benefits of pacifiers". Am Fam Physician. 79(8). :681-5. (2009)
- "The Right Age to Potty Train". https://web.archive.org/web/20221129194440/https://www.healthychildren.org/English/ages-stages/toddler/toilet-training/Pages/the-right-age-to-toilet-train.aspx. [2022-05-24]
- "Cognitive and Verbal Skills Needed for Toilet Training". https://web.archive.org/web/20221129193720/https://www.healthychildren.org/English/ages-stages/toddler/toilet-training/Pages/Cognitive-and-Verbal-Skills-Needed-for-Toilet-Training.aspx. [2009-11-02]
- "How Much Sleep Do I Need?". https://web.archive.org/web/20210913190430/https://www.cdc.gov/sleep/about_sleep/how_much_sleep.html
- Riley LK, Rupert J, Boucher O. "Nutrition in Toddlers". Am Fam Physician. 98(4). :227-233. (2018)
- Marcdante K, Kliegman RM. "Nelson Essentials of Pediatrics ". Elsevier. (2015). ISBN: 9781455759804
- Baker RD, Greer FR. "Diagnosis and Prevention of Iron Deficiency and Iron-Deficiency Anemia in Infants and Young Children (0–3 Years of Age)". Pediatrics. 126(5). :1040-1050. (2010)
- AAP Bright Futures. "Bright Futures Nutrition". American Academy of Pediatrics. (2011). ISBN: 9781581106244
- Am Fam Physician. "Giving Your Toddler the Best Nutrition". Am Fam Physician. 98(4). :Online. (2018)
- "Consensus Statement. Healthy Beverage Consumption in Early Childhood: Recommendations from Key National Health and Nutrition Organizations". https://healthyeatingresearch.org/wp-content/uploads/2019/09/HER-HealthyBeverage-ConsensusStatement.pdf. [2019-09-01]
- Nierengarten MB. "Special diets and supplements: Do’s and don’ts for children". Contemporary PEDS Journal. 37(1). :9-13. (2020)
- Ong C, Phuah K, Salazar E, How C. "Managing the ‘picky eater’ dilemma". Singapore Med J. 55(4). (2014)
- Clark MB, et al. "Fluoride Use in Caries Prevention in the Primary Care Setting". Pediatrics. 146(6). (2020)
- Segura A, Boulter S, et al. "Maintaining and Improving the Oral Health of Young Children". Pediatrics. 134(6). :1224-1229. (2014)
- Heyman MB, Abrams SA, Heitlinger LA, et al. "Fruit Juice in Infants, Children, and Adolescents: Current Recommendations". Pediatrics. 139(6). (2017)
- "Recommendations for using fluoride to prevent and control dental caries in the United States. Centers for Disease Control and Prevention". https://www.ncbi.nlm.nih.gov/pubmed/11521913. [2001-08-17]
- Davidson KW, Barry MJ, et al. "Screening and Interventions to Prevent Dental Caries in Children Younger Than 5 Years". JAMA. 326(21). :2172. (2021)
- Ntani G, Day PF, Baird J, et al. "Maternal and early life factors of tooth emergence patterns and number of teeth at 1 and 2 years of age". J Dev Orig Health Dis. 6(4). :299-307. (2015)
- Vohra R, Huntington S, Koike J, Le K, Geller R. "Pediatric Exposures to Topical Benzocaine Preparations Reported to a Statewide Poison Control System". West J Emerg Med. 18(5). :923-927. (2017)
- Poyak J. "Effects of pacifiers on early oral development". Int J Orthod Milwaukee. 17(4). :13-6
- Loh AR, Chiang MF. "Pediatric Vision Screening". Pediatr Rev. 39(5). :225-234. (2018)
- Lannering K, Bartos M, Mellander M. "Late Diagnosis of Coarctation Despite Prenatal Ultrasound and Postnatal Pulse Oximetry". Pediatrics. 136(2). :e406-e412. (2015)
- Maaks DLG, Starr NB, Brady MA, et al. "Burns' Pediatric Primary Care E-Book". Elsevier Health Sciences. (2019). ISBN: 9780323597142
- Kolon TF, Herndon CDA, Baker LA, et al. "Evaluation and Treatment of Cryptorchidism: AUA Guideline". J Urol. 192(2). :337-345. (2014)
- Zens T, Nichol PF, Cartmill R, Kohler JE. "Management of asymptomatic pediatric umbilical hernias: a systematic review". J Pediatr Surg. 52(11). :1723-1731. (2017)
- "WHO Growth Standards Are Recommended for Use in the U.S. for Infants and Children 0 to 2 Years of Age". https://web.archive.org/web/20230124201142/https://www.cdc.gov/growthcharts/who_charts.htm. [2010-09-09]
- Blaney SM, Giardino AP, Orange JS, et al. "Rudolph's Pediatrics, 23rd Edition". McGraw-Hill Education / Medical. (2018). ISBN: 9781259588594
- "CDC Growth Charts for the United States: Methods and Development". https://web.archive.org/web/20230316205321/https://www.cdc.gov/nchs/data/series/sr_11/sr11_246.pdf. [2002-05-01]
- Kliegman RM, Geme JS. "Nelson Textbook of Pediatrics, 2-Volume Set". Elsevier. :3623-3633. (2019). ISBN: 9780323529501
- Barstow C, Rerucha C. "Evaluation of short and tall stature in children". Am Fam Physician. 92(1). :43-50. (2015)
- "Measuring head circumference". https://web.archive.org/web/20230126185510/https://www.cdc.gov/zika/pdfs/microcephaly_measuring.pdf. [2016-09-08]
- Williams CA, Dagli A, Battaglia A. "Genetic disorders associated with macrocephaly". Am J Med Genet A. 146A(15). :2023-2037. (2008)
- Moini J, Oyindamola A, Ferdowsi K, Moini M. "Health Care Today in the United States". Elsevier. (2022). ISBN: 9780323993715
- "Predicting a Child’s Adult Height". https://web.archive.org/web/20230207173755/https://www.healthychildren.org/English/health-issues/conditions/Glands-Growth-Disorders/Pages/Predicting-a-Childs-Adult-Height.aspx. [2016-01-27]
- McInerny TK, Foy JM, Adam HM. "American Academy of Pediatrics Textbook of Pediatric Care". American Academy of Pediatrics. (2016). ISBN: 9781581109665
- DiTomasso D, Cloud M. "Systematic Review of Expected Weight Changes After Birth for Full-Term, Breastfed Newborns". J Obstet Gynecol Neonatal Nurs. 48(6). :593-603. (2019)
- Miller JR, Flaherman VJ, Schaefer EW, et al. "Early Weight Loss Nomograms for Formula Fed Newborns". Hosp Pediatr. 5(5). :263-268. (2015)
- Davis PJ, Cladis FP. "Smith's Anesthesia for Infants and Children E-Book". Elsevier Health Sciences. (2021). ISBN: 9780323698269
- Grossman DC, Bibbins-Domingo K, et al. "Screening for Obesity in Children and Adolescents: US Preventive Services Task Force Recommendation Statement". JAMA. 317(23). :2417. (2017)
- "Growth Chart Training : Using the WHO Growth Charts Case Example 4: Transitioning from the WHO Weight-for-Length Chart to the CDC BMI-for-Age Chart at Age 2 Years". https://web.archive.org/web/20230207180111/https://www.cdc.gov/nccdphp/dnpao/growthcharts/who/examples/example4.htm. [2022-01-13]
- Accogli A, Geraldo AF, Piccolo G, et al. "Diagnostic Approach to Macrocephaly in Children". Front Pediatr. 9. (2022)
- The Joint Committee on Infant Hearing. "Year 2019 Position Statement: Principles and Guidelines for Early Hearing Detection and Intervention Programs". Journal of Early Hearing Detection and Intervention. 4(2). :1-44. (2019)
- Yoeli JK, Nicklas D. "Hearing Screening in Pediatric Primary Care". Pediatr Rev. 42(5). :275-277. (2021)
- "American Academy of Audiology Childhood Hearing Screening Guidelines". https://audiology-web.s3.amazonaws.com/migrated/ChildhoodScreeningGuidelines.pdf_5399751c9ec216.42663963.pdf. [2011-09-01]
- "Hearing loss in children. Screening and diagnosis of hearing loss". https://web.archive.org/web/20221118193101/https://www.cdc.gov/ncbddd/hearingloss/screening.html#:%E2%88%BC:text=All%20babies%20should%20be%20screened,than%203%20months%20of%20age.. [2022-06-18]
- American academy of pediatrics section on ophthalmology, American association for pediatric ophthalmology and strabismus, American academy of ophthalmology, American association of certified orthoptists. "Red Reflex Examination in Neonates, Infants, and Children". Pediatrics. 122(6). :1401-1404. (2008)
- Simon GR, Boudreau ADA, et al. "Visual System Assessment in Infants, Children, and Young Adults by Pediatricians (reaffirmed 2021)". Pediatrics. 137(1). (2016)
- Grossman DC, Curry SJ, et al. "Vision Screening in Children Aged 6 Months to 5 Years". JAMA. 318(9). :836. (2017)
- "Vision Screening for Infants and Children Joint Policy Statement". https://web.archive.org/web/20241121172349/https://www.aao.org/education/clinical-statement/vision-screening-infants-children-2022. [2022-10-01]
- Donahue SP, Baker CN, Simon GR, et al. "Procedures for the Evaluation of the Visual System by Pediatricians (reaffirmed 2022)". Pediatrics. 137(1). (2016)
- "Vision Screening Recommendations". https://web.archive.org/web/20221109192345/https://aapos.org/members/vision-screening-guidelines. [2022-01-01]
- American Academy of Pediatrics. "Instrument-Based Vision Screening in Children". Pediatrics. 139(1). (2017)
- Grossman DC, Curry SJ, et al. "Screening for Adolescent Idiopathic Scoliosis". JAMA. 319(2). :165. (2018)
- Am Fam Physician. "Screening for Adolescent Idiopathic Scoliosis: Recommendation Statement". Am Fam Physician. 97(10). (2018)
- Hresko MT, Talwalkar V, Schwend R. "Early Detection of Idiopathic Scoliosis in Adolescents". J Bone Joint Surg. 98(16). :e67. (2016)
- Flynn et al. "Clinical Practice Guideline for Screening and Management of High Blood Pressure in Children and Adolescents". Pediatrics. 140(3). (2017)
- "Vision Screening for Infants and Children - 2022. Joint Policy Statement". https://web.archive.org/web/20221129174046/https://www.aao.org/clinical-statement/vision-screening-infants-children-2022. [2022-10-01]
- Joint Comittee on Infant Hearing. "Year 2007 Position Statement: Principles and Guidelines for Early Hearing Detection and Intervention Programs". Pediatrics. 120(4). :898-921. (2007)
- Hyman SL, Levy SE, Myers SM, et al. "Identification, Evaluation, and Management of Children With Autism Spectrum Disorder". Pediatrics. 145(1). (2020)
- Gitterman BA, Flanagan PJ, et al. "Poverty and Child Health in the United States". Pediatrics. 137(4). (2016)
- Sokol R, Austin A, Chandler C, et al. "Screening Children for Social Determinants of Health: A Systematic Review". Pediatrics. 144(4). (2019)
- Mangione CM, Barry MJ, et al. "Screening for Anxiety in Children and Adolescents". JAMA. 328(14). :1438. (2022)
- Mangione CM, Barry MJ, et al. "Screening for Depression and Suicide Risk in Children and Adolescents". JAMA. (2022)
- "Childhood Lead Poisoning Prevention - Recommended Actions Based on Blood Lead Level". https://web.archive.org/web/20250912133533/https://www.cdc.gov/lead-prevention/hcp/clinical-guidance/?CDC_AAref_Val=https://www.cdc.gov/nceh/lead/advisory/acclpp/actions-blls.htm. [2025-08-21]
- Lanphear BP, Lowry JA, et al. "Prevention of Childhood Lead Toxicity". Pediatrics. 138(1). (2016)
- Mayans L. "Lead Poisoning in Children". Am Fam Physician. 100(1). :24-30. (2019)
- "Lead - Refugee Health Domestic Guidance". https://web.archive.org/web/20250915071127/https://www.cdc.gov/immigrant-refugee-health/hcp/domestic-guidance/lead.html. [2024-05-15]
- National Heart, Lung, and Blood Institute. "Expert Panel on Integrated Guidelines for Cardiovascular Health and Risk Reduction in Children and Adolescents: Summary Report". Pediatrics. 128(Supplement). :S213-S256. (2011)
- Nolt D, Starke JR. "Tuberculosis Infection in Children and Adolescents: Testing and Treatment". Pediatrics. 148(6). (2021)
- Erickson CC, Salerno JC, Berger S, et al. "Sudden Death in the Young: Information for the Primary Care Provider". Pediatrics. 148(1). (2021)
- Lipkin PH, Macias MM, Norwood KW, et al. "Promoting Optimal Development: Identifying Infants and Young Children With Developmental Disorders Through Developmental Surveillance and Screening". Pediatrics. 145(1). (2020)
- Johnson CP, Myers SM. "Identification and Evaluation of Children With Autism Spectrum Disorders". Pediatrics. 120(5). :1183-1215. (2007)
- "Contributor Disclosures - Well-child visits. All of the relevant financial relationships listed for the following individuals have been mitigated: Jan Schlebes (medical editor, is a shareholder in Fresenius SE & Co KGaA). None of the other individuals in control of the content for this article reported relevant financial relationships with ineligible companies. For details, please review our full conflict of interest (COI) policy"