Summary
Wounds are a break in the skin and/or a disruption of the skin's normal barrier function. Wound healing is a step-wise cellular response involving fibroblasts, macrophages, endothelial cells, and keratinocytes that restore the structural and functional integrity of the skin. The four general stages of wound healing are exudative, resorptive, proliferative, and maturation. While the three initial stages take place within the first two weeks, the last stage proceeds over months. Many factors affect wound healing, including the size of the wound, tension on wound edges, the presence of foreign bodies or infection, and the baseline health and nutrition of the patient. In addition, chronic health conditions such as diabetes and peripheral vascular disease can slow the wound healing process. Delayed wound healing may lead to the formation of a chronic wound.
Phases of wound healing
| Phases of wound healing [1] | ||||
|---|---|---|---|---|
| Phase | Timing | Cells involved | Characteristics | Involved tissue mediators |
| Exudative |
|
|
|
|
| Resorptive |
|
|
|
|
| Proliferative |
|
|
|
|
| Maturation |
|
|
|
|




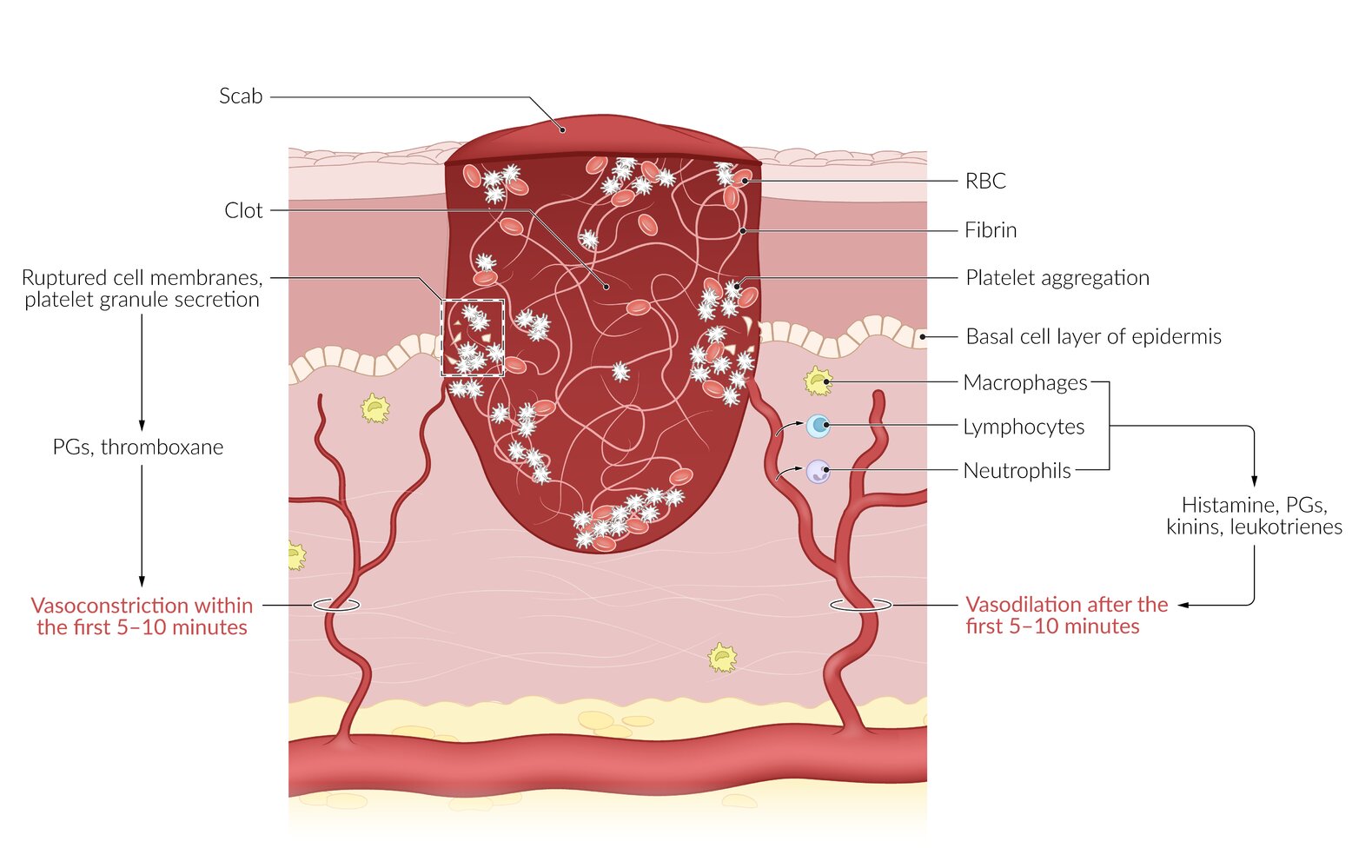
Within the wound area, damaged blood vessels cause hemostasis via platelet activation. Platelets secrete prostaglandins (PGs) and thromboxane, leading to vasoconstriction within the first 5–10 minutes. After this, vasodilation is mediated by histamine, PGs, kinins and, leukotrienes, supporting the invasion of leukocytes.
© AMBOSS
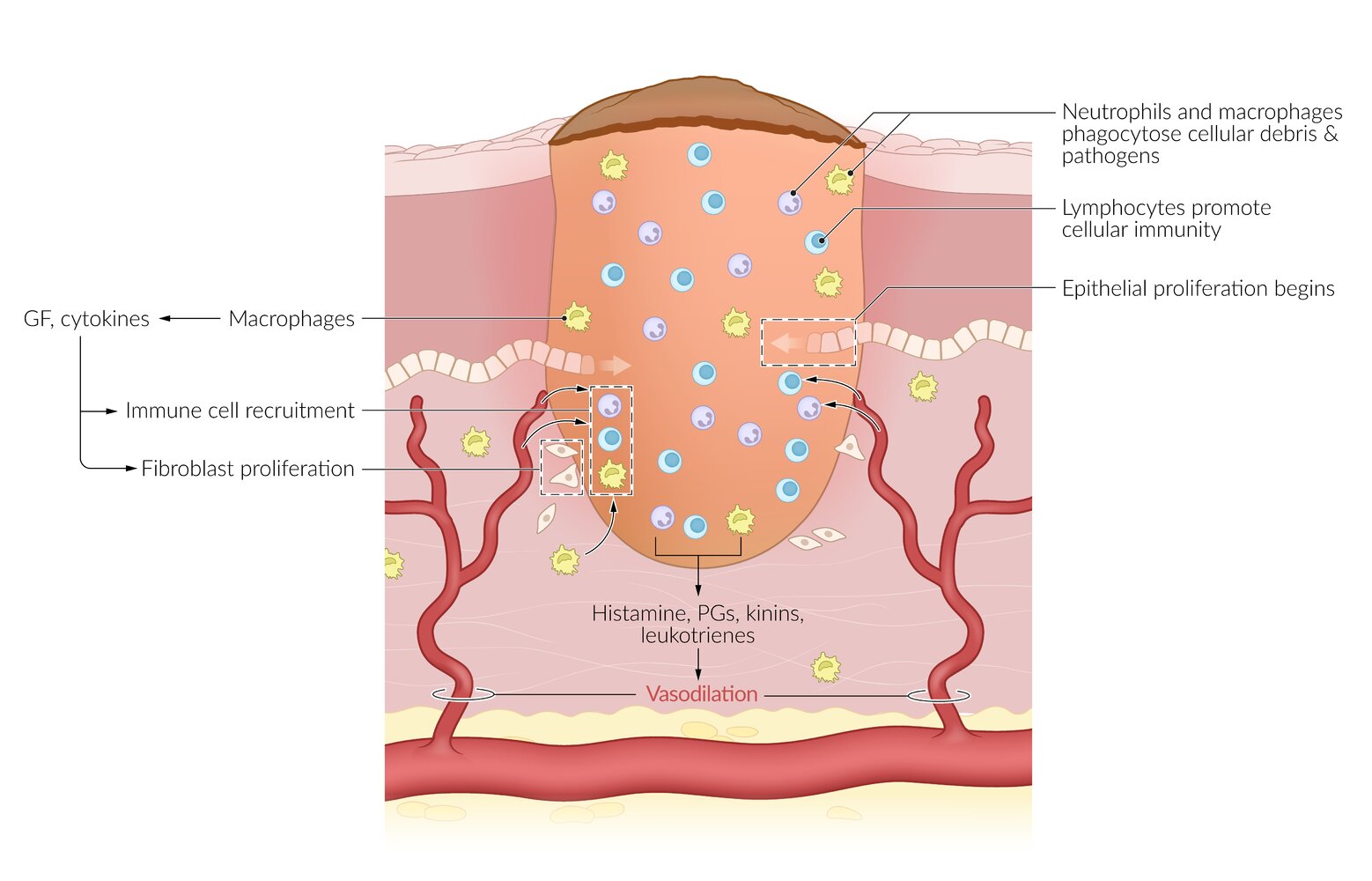
Macrophages release growth factors and cytokines that recruit other immune cells and stimulate fibroblast proliferation. Lymphocytes promote cellular immunity, and neutrophils and macrophages phagocytose pathogens and cellular debris.
© AMBOSS
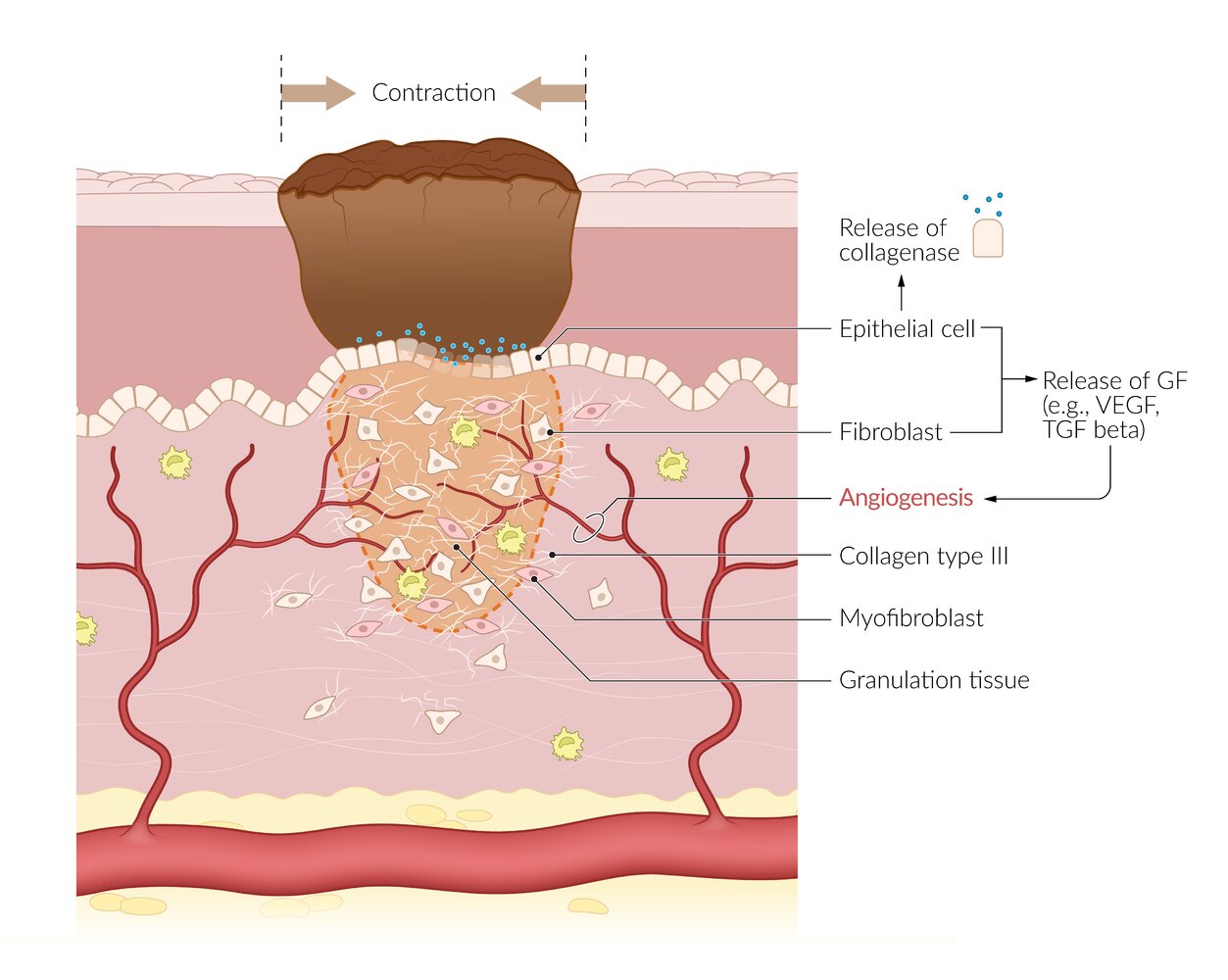
Granulation tissue develops during the proliferative stage. It consists of macrophages, fibroblasts, and lymphocytes. Granulation tissue is abundant in blood capillaries and type 3 collagen fibers. Epidermal stem cells at the wound margins proliferate to renew the epidermis at the wound site. Secretion of collagenase facilitates clot degradation. Wound contraction occurs as collagen synthesis increases and pulls the wound edges together. This process is facilitated by myofibroblasts.
© AMBOSS
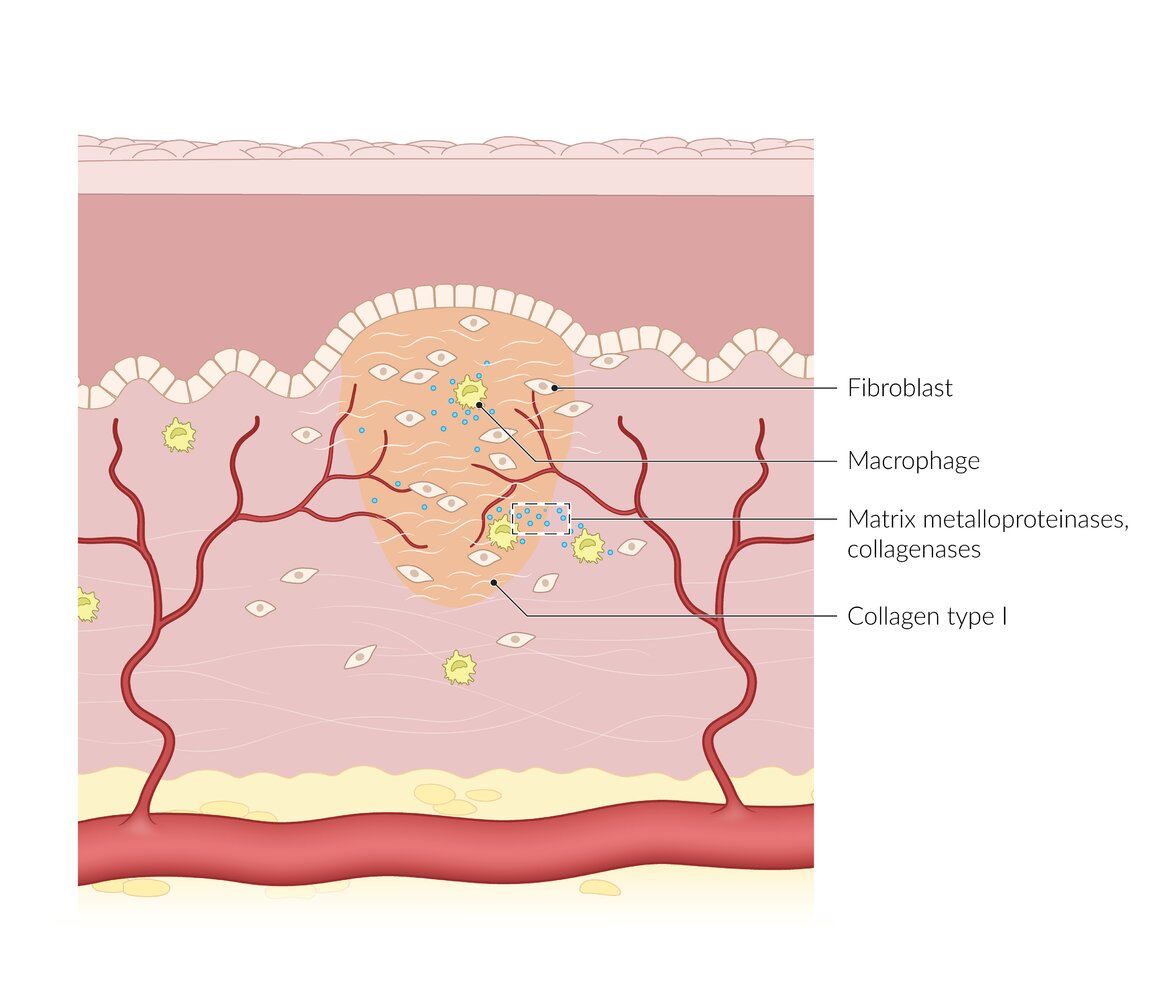
Scar tissue formation occurs as type I collagen replaces type III collagen in the connective tissue. The scar tissue is covered by epidermis, but it lacks melanocytes and skin appendages such as hair follicles or cutaneous sweat glands.
© AMBOSS
Wound healing complications
Scar formation
- Occurs when initial injury cannot be repaired solely by cell regeneration
- Cells that cannot be regenerated (e.g., due to chronic injury or because acute injury is too severe) are replaced by connective tissue.
- After 3 months, 70–80% of tensile strength is regained. [2]
- Maximum strength of scar tissue is approx. 80% of that of unwounded skin. [2]
Excessive scar
- Dysregulation of the wound healing process during the proliferative stage and maturation stage leads to excess fibroblast replication and collagen deposition.
- Molecular mechanisms [3][4][5][6][7][8]
-
Increased production of:
- Certain isoforms of transforming growth factor-beta (primary mediator)
- Connective tissue growth factor
- Platelet-derived growth factor
- Tissue inhibitors of metalloproteinases
- Decreased production of:
- Basic fibroblast growth factor
- Metalloproteinases (e.g., collagenase)
- Interleukin-10
-
Increased production of:
Hypertrophic scar
- Cutaneous condition characterized by high fibroblast proliferation and collagen production that leads to a raised scar that does not grow beyond the boundaries of the original lesion.
- See “Hypertrophic scars.”
Keloid
- Skin lesions caused by high fibroblast proliferation and collagen production in excessive tissue response to typically small skin injuries
- Lesions grow beyond the original wound margins, leading to a ”claw-like” appearance.
- See “Keloid scars.”
Contracture
- Excessive proliferation in myofibroblasts during proliferative and maturation phases leads to contraction of the wound.
- Excessive contraction can reduce the functionality of the injured limbs or organs.
- Wounds that cross a joint (e.g., on the hands and fingers) are at high risk for causing functional deficits from contracture. Periodic exercise of the involved limb can help preserve normal function.
References
- Stadelmann WK, Digenis AG, Tobin GR. "Physiology and healing dynamics of chronic cutaneous wounds". Am J Surg. 176(2A Suppl). :26S-38S. (1998)
- Thiruvoth F, Mohapatra D, Sivakumar D, Chittoria R, Nandhagopal V. "Current concepts in the physiology of adult wound healing". Plastic and Aesthetic Research. 2(5). :250. (2015)
- Zhu Z, Ding J, Tredget EE. "The molecular basis of hypertrophic scars.". Burns & trauma. 4. :2. (2016)
- Leivonen SK, Lazaridis K, Decock J, et al. "TGF-β-elicited induction of tissue inhibitor of metalloproteinases (TIMP)-3 expression in fibroblasts involves complex interplay between Smad3, p38α, and ERK1/2.". PloS one. 8(2). :e57474. (2013)
- Shah M, Foreman DM, Ferguson MW. "Neutralisation of TGF-beta 1 and TGF-beta 2 or exogenous addition of TGF-beta 3 to cutaneous rat wounds reduces scarring.". J Cell Sci. 108 ( Pt 3). :985-1002. (1995)
- Schultz GS, Chin GA, Moldawer L, et al. "Principles of Wound Healing". StatPearls. (2011)
- Köse O, Waseem A. "Keloids and hypertrophic scars: are they two different sides of the same coin?". Dermatol Surg. 34(3). :336-46. (2008)
- Verhaegen PD, van Zuijlen PP, Pennings NM, et al. "Differences in collagen architecture between keloid, hypertrophic scar, normotrophic scar, and normal skin: An objective histopathological analysis.". Wound Repair Regen. 17(5). :649-56